Florida Surgeon General Dr. Joseph Ladapo
Tuesday, October 26, 2021
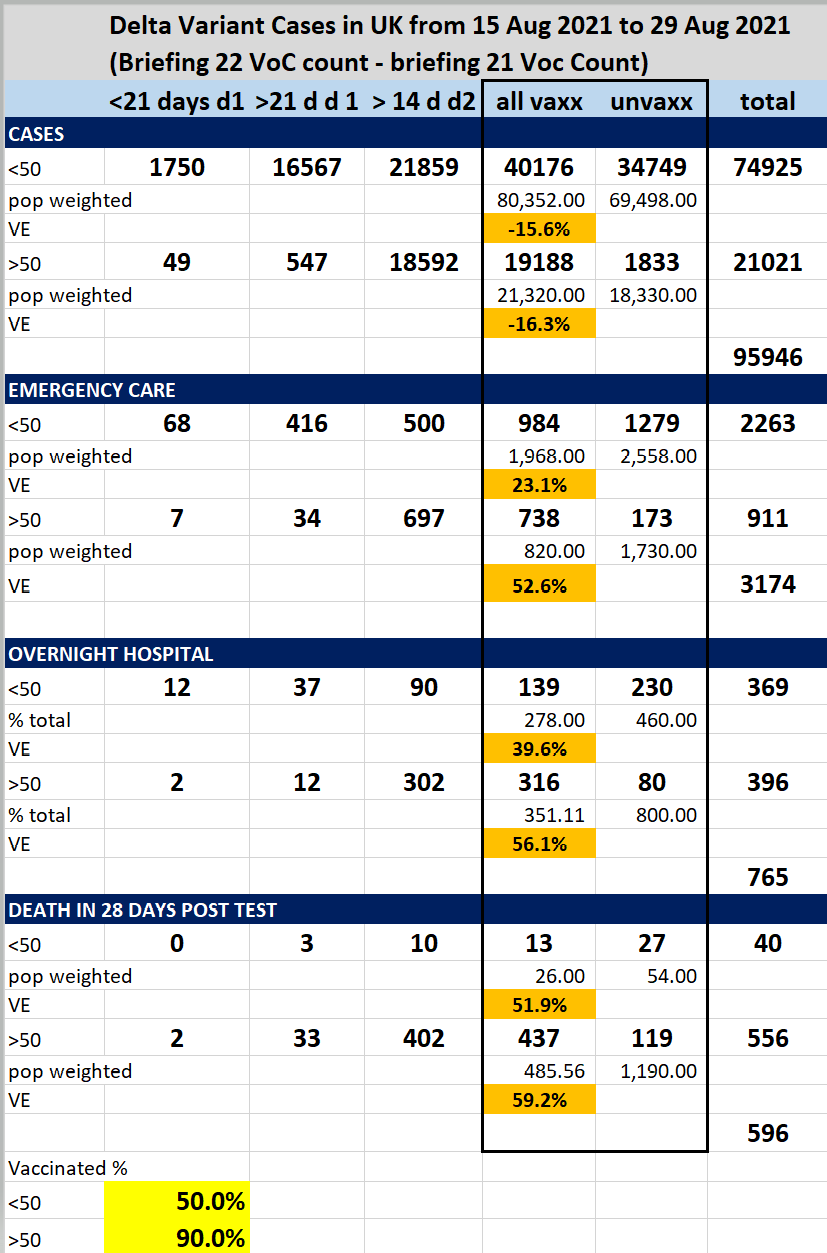
Updated: Death to Vaccination Charts
This was done recently by John Hopkins Hospital
It's pretty much a continuing story as several have done similar comparisons earlier
Or even earlier
Monday, October 25, 2021
FDA committee meets to debate and vote on Covid booster shots for Ages 5-11
7 1/2 hour meeting by the FDA
FDA Penal says benefits outweigh the risks
They passed it unanimously. Here are some alarming highlights
Steve Kirsch on Children Vaccine Adverse Effects
"We're never going to know how safe it is until we give it"
"Cases of Myocarditis higher than hospitalizations from COVID"
Sunday, October 24, 2021
Ten red flags in the FDA's risk-benefit analysis of Pfizer's EUA application to inject American children 5 to 11 with its mRNA product
The FDA briefing document is preposterous junk science and it must be withdrawn immediately
Where to even begin with the FDA’s preposterous risk-benefit analysis of Pfizer’s mRNA COVID-19 “vaccine” in children ages 5 to 11?
Let’s start with my bona fides. I have a year of undergraduate statistics at one of the best liberal arts colleges in America (Swarthmore). I have a year of graduate statistics at the masters program rated #1 for policy analysis (UC Berkeley). And I have a Ph.D. in political economy from one of the top universities in the world (University of Sydney). My research focus is on corruption in the pharmaceutical industry so I’ve read scientific studies in connection with vaccines nearly every day for 5 years. Earlier in my career I worked professionally tearing apart shoddy cost-benefit analyses prepared by corporations that were trying to get tax breaks, contracts, and other concessions from local government. Suffice it to say I’ve thought a lot about risk-benefit analysis and I’m better equipped than most to read one of these documents.
The FDA’s risk-benefit analysis in connection with Pfizer’s Emergency Use Authorization (EUA) application to inject children ages 5 to 11 with their COVID-19 vaccine is one of the shoddiest documents I’ve ever seen.
Let’s take it from the top:
🚩 COVID-19 rates in children ages 5 to 11 are so low that there were ZERO cases of severe COVID-19 and ZERO cases of death from COVID in either the treatment (n= 1,518) or control group (n= 750). So any claims you see in the press about the Pfizer vaccine being “90% effective” in children are meaningless because they are referring to mild cases from which children usually recover quickly (and then have robust broad spectrum immunity). So there is literally no emergency in this population for which one could apply for Emergency Use Authorization. Pfizer’s application should be dead on arrival if the FDA actually followed the science and their own rules. We will return to this topic below.
🚩 Pfizer’s clinical trial in kids was intentionally undersized to hide harms. This is a well known trick of the pharmaceutical industry. The FDA even called them out on it earlier this summer and asked Pfizer to expand the trial and Pfizer just ignored them because they can. (Pfizer fudged it by importing data from a different study but this other study only monitored adverse outcomes for 17 days so if anything the new data polluted rather than clarified outcomes). To put it simply, if the rate of particular adverse outcome in kids as a result of this shot is 1 in 5,000 and the trial only enrolls 1,518 in the treatment group then one is unlikely to spot this particular harm in the clinical trial. Voilà “Safe & Effective(TM)”.
🚩 Pfizer only enrolled “participants 5-11 years of age without evidence of prior SARS-CoV-2 infection.” Does the Pfizer mRNA shot wipe out natural immunity and leave one worse-off than doing nothing as shown in this data from the British government? Pfizer has no idea because children with prior SARS-CoV-2 infection were excluded from this trial. This was by design. Toxic polluters have learned to not ask questions that they do not want the answers to, lest they wind up staring at their own smoking gun in a future court case.
According to an analysis by Alex Berenson:
“What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus. Specifically, vaccinated people don’t seem to be producing antibodies to the nucleocapsid protein, the shell of the virus, which are a crucial part of the response in unvaccinated people. This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE (or more than once, probably). It also means the virus is likely to select for mutations that go in exactly that direction because those will essentially give it an enormous vulnerable population to infect. And it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.”
🚩 Did Pfizer LOSE CONTACT with 4.9% of their clinical trial participants? The FDA risk-benefit document states: “Among Cohort 1 participants, 95.1% had safety follow-up ≥2 months after Dose 2 at the time of the September 6, 2021 data cutoff.” So what happened with those 4.9% who did not have safety follow-up 2 months after Dose 2? Were they in the treatment or control group? We have no idea because Pfizer isn’t saying. Given the small size of the trial, failing to follow up with 4.9% of the participants potentially skews the results.
🚩 The follow up period was intentionally too short. This is another well-know trick of the pharmaceutical industry designed to hide harms. Cohort 1 appears to have been followed for 2 months, cohort 2 was only monitored for adverse events for 17 days. Many harms from vaccines including cancer and autoimmune disorders take much longer to show up. As the old saying goes, “you can have it quick or you can have it done right, but you cannot have both.” Pfizer chose quick.
🚩 The risk-benefit model created by the FDA only looks at one known harm from the Pfizer mRNA shot — myocarditis. But we know that the real world harms from the Pfizer mRNA shot go well beyond myocarditis and include anaphylaxis, Bell’s Palsy, heart attack, thrombocytopenia/ low platelet, permanent disability, shingles, and Guillain-Barré Syndrome (GBS) to name a few. Cancer, diabetes, endocrine disruption, and autoimmune disorders may show up later. But the FDA does not care about any of that because they have a vaccine to sell so they just ignore all of those factors in their model.
🚩 Pfizer intentionally wipes out the control group as soon as they can by vaccinating all of the kids who initially got the placebo. They claim that they are doing this for “ethical reasons”. But everyone knows that Pfizer’s true aim is to wipe out any comparison group so that there can be no long term safety studies. Wiping out the control group is a criminal act and yet Pfizer, Moderna, J&J, and AZ do this as standard practice with the blessing of the FDA/CDC.
🚩 Given all of the above, how on earth did the FDA claim any benefits at all from this shot? You should probably sit down for this part because it’s a doozy! Here’s the key sentence:
Vaccine effectiveness was inferred by immunobridging SARS-CoV-2 50% neutralizing antibody titers (NT50, SARS-CoV-2 mNG microneutralization assay).
Wait, what!? I’ll explain. There were ZERO cases of severe COVID-19 in the clinical trial of children ages 5 to 11. So Pfizer and the FDA just ignored all of the actual health outcomes (they had to, there is no emergency, so the application is moot). INSTEAD Pfizer switched to looking at antibodies in the blood. In general, antibodies are a poor predictor of immunity. And the antibodies in the blood of these 5 to 11 year old children tell us nothing because again, there were zero cases of severe COVID-19 in this study (none in the treatment group, none in the control group). So Pfizer had to get creative! What they came up with is “immuno-bridging”. Pfizer looked at the level of antibodies in the bloodwork of another study, this one involving people 16 to 25 years old, figured out the level of antibodies that seems to be protective in that population, then figured out how many kids ages 5 to 11 had similar levels of antibodies in their blood, and then came up with a number for how many cases, hospitalizations, ICU admissions, and deaths would be prevented by this shot in the 5 to 11 population in the future, based on the antibody levels and health outcomes from the 16 to 25 year old population. If your head hurts from that tortured logic, it should, because such chicanery is unprecedented in a risk-benefit analysis.
So when the FDA uses this tortured logic at the beginning of their briefing document, all of the calculations that stem from this will be flat out wrong. Not just wrong but preposterous and criminally wrong.
The whole ballgame comes down to Table 14 on page 34 of the FDA’s risk-benefit document. And there the red flags come fast and furious.
🚩 The FDA model only assesses the benefits of vaccine protection in a 6-month period after completion of two doses. Furthermore it assumes constant vaccine efficacy during that time period. This is problematic on several counts.
First, reducing mild cases in children is not a desired clinical outcome. As Dr. Geert Vanden Bossche points out, mass vaccination turns kids into shedders of more infectious variants.
"Under no circumstances should young and healthy people be vaccinated as it will only erode their protective innate immunity towards Coronaviruses (CoV) and other respiratory viruses. Their innate immunity normally/ naturally largely protects them and provides a kind of herd immunity in that it dilutes infectious CoV pressure at the level of the population, whereas mass vaccination turns them into shedders of more infectious variants. Children/ youngsters who get the disease mostly develop mild to moderate disease and as a result continue to contribute to herd immunity by developing broad and long-lived immunity. If you are vaccinated and get the disease, you may develop life-long immunity too but why would you take the risk of getting vaccinated, especially when you’re young and healthy? Firstly, there is the risk of potential side effects; secondarily, there is the ever increasing risk that your vaccinal antibodies will no longer be functional while still binding to the virus, thereby increasing the likelihood of ADE or even severe disease...."
Second, we know that vaccine efficacy in the month after the first dose is negative because it suppresses the immune system and it begins to wane after 4 months so all of the FDA’s estimates of vaccine efficacy are inflated.
Third, the harms of myocarditis from these shots will likely unfold over the course of years. Robert Malone, the inventor of mRNA technology notes that the FDA is admitting that children will be injected twice a year forever (hence the six month time frame in the FDA risk-benefit model). But the risks of “adverse events such as cardiomyopathy will be cumulative.” So any model that only looks at a six month time frame is hiding the true adverse event rate.
🚩 The FDA/Pfizer play fast and loose with their estimates of myocarditis. First they estimate “excess” (read: caused by the shot) myocarditis using data from the private “Optum health claim database” instead of the public VAERS system (p. 32). So it’s impossible for the public to verify their claims. Then, when it comes to estimating how many children with vaccine-induced myocarditis will be hospitalized and admitted to the ICU they use the Vaccine Safety Datalink (see page 33). Why switch to a different database for those estimates? Finally, there is no explanation for how they calculated “excess” myocarditis deaths, so they just put 0. Red flag, red flag, red flag.
The FDA estimates that there will be 106 extra myocarditis cases per 1 million double-jabbed children 5-11. There are 28,384,878 children ages 5 to 11 in the U.S. The Biden administration wants to inject Pfizer mRNA shots into all of them and has already purchased enough doses to do just that (even though only 1/3rd of parents want to jab their kids with this shot). So (if the Biden administration has its way) 106 excess myocarditis cases per 1 million x 28.38 million people would be 3,009 excess myocarditis cases post-vaccination if the Pfizer vaccine is approved.
And over the course of several years many of those children will die. Dr. Anthony Hinton (“Consultant Surgeon with 30 years experience in the NHS”) points out that myocarditis has a 20% fatality rate after 2 years and a 50% fatality rate after 5 years.

So the FDA has it exactly backwards — they want to prevent mild COVID in children which reduces herd immunity and they just flat out lie about the harms from myocarditis.
I’ve taken the liberty to correct the FDA’s Table 14 with actual real world data and extended it over 5 years. It looks like this:

A study by Harvard Pilgrim Healthcare for the U.S. Department of Health and Human Services estimated that VAERS only captured 1% of actual vaccine injuries. Steve Kirsch has done elaborate modeling that puts the Under-Reporting Factor of COVID-19 vaccine deaths at 41 (so multiply the above numbers by 41). And myocarditis is just one of a multitude of possible harms from COVID-19 vaccines. Dr. Jessica Rose recently calculated an Under-Reporting Factor of 31 for all severe adverse events following vaccination.
Conclusion
The Pfizer vaccine fails any honest risk-benefit assessment in connection with its use in children ages 5 to 11. The FDA’s risk-benefit analysis of Pfizer’s mRNA vaccine in children ages 5 to 11 is shoddy. It used tortured logic (that would be rejected by any proper academic journal) in order to reach a predetermined result that is not based in science. The FDA briefing document is a work of fiction and it must be withdrawn immediately. If the FDA continues with this grotesque charade it will cause irreparable harms to children and the FDA leadership will one day be prosecuted for crimes against humanity.
🚩 An astute reader pointed out that on page 14, the FDA explains that Pfizer has changed the ingredients in their mRNA vaccine. They write:
To provide a vaccine with an improved stability profile, the Pfizer-BioNTech COVID-19 Vaccine for use in children 5-11 years of age uses tromethamine (Tris) buffer instead of the phosphate-buffered saline (PBS) as used in the previous formulation and excludes sodium chloride and potassium chloride.
I’m deeply skeptical of this account (I doubt this has anything to do with an “improved stability profile”) and invite others to weigh in on this. I also recall that tromethamine has a long and troubled history and invite readers to dig into this further (I’m happy to post additional links as they become available).
This is a live article. The FDA only gives the public 2 days to review meeting materials so I had to publish this article immediately. If you spot any errors please let me know and I will correct them. If you find additional flaws in the FDA’s risk-benefit analysis please post them in the comments so that I may add them.
Sunday, October 17, 2021
How Long Do The Vaccinated Have To Live?
How Long Do the Vaxinated Have To Live?
By Steven Fishman
I deferred this question to a friend of mine, Dr. Mylo Canderian, Ph.D. [born Milos Iskanderianos, Corfu, Greece, 1938], who developed the patent for Graphene Oxide for use as a Hematological Bioweapon in 2015.
In full transparency, Dr. Canderian is what I would call a “Genocidal Globalist,” who follows Precept Ten of the Georgia Guidestones, which is very seldom discussed, stating “Be not a Cancer upon the Earth; Leave Room for Nature.”
Dr. Canderian is a Medical Contributor to the World Health Organization and is also very supportive of Klaus Schwab and the “Great Reset,” ushering in one world digital currency which is a secondary goal of the WHO for 2022.
Dr. Canderian is of the opinion that 95% of the world’s population are “Useless Eaters” who need to be euthanized as quickly as possible.
“Look at downtown Chicago, Baltimore, or Los Angeles,” he has stated, “and you will clearly see why the Useless Eaters must be put down like rabid dogs.”
He has expressed his disdain for “Infectious Educators” who promote Critical Race Theory, and is confident that the “vaccine” will put an end to “Human Cancer Upon the Earth.”
Dr. Canderian is an ardent supporter of Freemasonry’s Duty and Obligation to rid the world of the “Plague of Humanity.”
Yet on a personal level, he and I share a passion for the same exotic dish served at L’emince de Veau in Geneva: Cream of Hummingbird Soup followed by Elk Tongue.
We both are fans of Chef Gaston Sere de Rivieres, who is a culinary genius.
So, I asked Mylo, “How can the “vaccinated” know with certainty how long they have to live once they have been jabbed?”
He presented me with the information, called the “End of Cycle Formula.”
He explained how easy it is to calculate.
“The Power of Simplicity,” he said. “There is a maximum cycle of ten years from injection to End of Cycle,” [or death], he elaborated. “And it is extremely easy to determine.”
He said any hematologist can see it within seconds under a microscope, and even more readily under an electron microscope. “The percentage of blood affected [or contaminated] by or with Graphene Oxide is the reciprocity of the End of Cycle calculation,” he divulged.
In other words, an “inoculatee” [as he calls anyone jabbed with the Experimental Use Authorization Eugenics Depopulation Lethal Injection Bioweapon] having 20% Graphene Oxide deterioration in their blood will, barring any other input criteria, live for 8 years. [10 years less 20%].
Someone with 70% Graphene Oxide deterioration will not live more than 3 years. [10 years less 70%].
Dr. Jane Ruby recently was interviewed by Stew Peters on his podcast and showed examples of what the deteriorated blood looks like when exposed to Graphene Oxide.
Graphene Oxide, for those who are unaware, is the component of Messenger RNA spike proteins and prions, which is at war with the heart, lungs, brain and blood for oxygen.
Graphene Oxide is an oxygen sponge which deprives the body of necessary oxygen and causes many complications, including but not limited to anaphylactic shock, toxic blood clotting, fatal lung paralysis, mitochondrial cancer, and endothelial cancer.”
Dr. Mylo Canderian’s viewpoint is much the same as Klaus Schwab, Bill Gates, and the Big Pharma CEO’s: LET THEM ALL DIE!
I asked Mylo what the effect of second and third shots and boosters do and how that changes the End of Cycle table.
Mylo replied: “It is all measurable through hematological testing. The more shots and boosters the imbeciles get, the worse their blood will look under a microscope, and the quicker they will turn to fertilizer.”
Finally, I asked him how the plot to kill so many billions of people could be kept so secret by such a group of elites.
His answer was: “You don’t know much about Freemasonry, do you, Steve?”
And there you have it.
Thursday, October 14, 2021
Heroes of the Pandemic
Meet 15 of the leading physicians and scientists at the forefront of the counter-narrative on COVID-19.
By Debra Heine
October 2, 2021
Many highly accomplished and credentialed medical professionals have put their careers and reputations on the line with their public opposition to the failed COVID strategies of the global biomedical complex. For this, the corporate media has done everything it can to discredit them, and suppress their alternative message.
Over 9,100 medical doctors and scientists have signed a document charging policy-makers with potential “crimes against humanity,” accusing them of preventing physicians from providing life-saving treatments for their patients and suppressing open scientific discussion.
The now-famous “Rome Declaration” wasn’t even the first time a large number of medical experts had gone on the record to reject the tenets of the church of COVID.
A year ago, more than 860,000 infectious disease epidemiologists and public health scientists signed a declaration expressing their “grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies.”
The Great Barrington Declaration argued that “the most compassionate” way to reach herd immunity while minimizing mortality and social harm was “to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk.”
Unfortunately, because of the work they’ve done over the past year and a half advocating for early treatments, and raising red flags about the experimental vaccines, many brave doctors and scientists have had their voices muzzled and their reputations smeared by the corporate media.
Why? Because no one is allowed to question the official narrative of the global biomedical complex, which is that the vaccines are very safe, effective, and the best way to fight COVID-19.
Among the detractors of this narrative, highlighted below, are medical doctors, infectious-disease researchers, virologists, a former vice president of Pfizer, the inventor of mRNA vaccine technology, and even a state surgeon general.
Even as the authoritarian Biden Administration has ratcheted up pressure on unvaccinated Americans to get the jab or lose all of their rights, these bold medical professionals have fought back, arguing that the experimental injections fail a risk-benefit assessment for most people, and are arguably a violation of the Nuremberg Code.
Analysis from the Vaccine Adverse Event Reporting System (VAERS) data shows that over a half a million people have had adverse effects from the vaccines, including life-threatening reactions, permanent disability, birth defects, and death. For a variety of reasons, (e.g. deliberate suppression of the truth, laziness) it is widely believed that only a small fraction of adverse events actually get reported into the system. A 2011 study by Harvard Pilgrim Health Care, for instance, found that the number could be as low as one percent.
Forty-five years ago, the federal government pulled a vaccine that caused only a tiny fraction of the number of adverse reactions that are being reported today.
In 1976, three states halted the Swine Flu vaccine after only three deaths. Later that year, the CDC pulled the vaccine from the market entirely after about 500 people developed a rare neurological condition called Guillain-Barré syndrome, and about 25 people died.
The number of COVID vaccine casualties in 2021 eclipsed those numbers in the first month.
The following 15 doctors and scientists have been standout heroes of the pandemic, using their influence to push back against the global medical establishment narrative by trumpeting “off-label” treatments to fight COVID-19, and waving red flags over the vaccines.
These experts don’t agree on everything. For instance, some say the jabs are not “vaccines,” they’re gene therapies. Dr. Robert Malone, the inventor of mRNA medical technology, disputes this. There is also disagreement on whether there is asymptomatic spread. Dr. Michael Yeadon has said there is none, while others say there is asymptomatic spread, albeit with a lesser viral load.
Virtually all of these brilliant and brave individuals have been “corrected” by non-credentialed “fact-checkers” who cite federally funded medical authorities like the National Institutes of Health or the Centers for Disease Control and Prevention to refute their work. But all these doctors have contributed valuable information and insights into the pandemic that should not be hidden from the people.
Dr. Robert Malone
Dr. Robert Malone is a medical doctor and an infectious-disease researcher, and is recognized as the discoverer of in-vitro and in-vivo RNA transfection and the inventor of mRNA vaccines while he was at the Salk Institute in 1988. His research was continued at Vical in 1989, where the first in-vivo mammalian experiments were designed by him. Between 1988 and 1989, the doctor wrote the patent disclosures for mRNA vaccines.
These days Malone worries that his discovery has led to the government forcing injections on people that may be making COVID-19 infections worse.
Malone contracted the virus in February 2020, and got the Moderna vaccine in 2021 hoping that it would alleviate his long-COVID symptoms. Alas, it made things worse. Among other complaints, he says he still has a cough and is dealing with hypertension and reduced stamina. “My body will never be the same,” he told Atlantic reporter Tom Bartlett.
On June 10, Malone joined computer science entrepreneur Steve Kirsch and biologist Bret Weinstein on the Dark Horse Podcast. During the discussion, Malone raised numerous safety concerns with the Pfizer-BioNTech and Moderna COVID-19 vaccines, both of which use the mRNA technology he pioneered. He also warned of future autoimmune issues caused by the spike proteins within the mRNA injections.
Malone also asserted that the Food and Drug Administration (FDA) was aware that the spike proteins were “biologically active and could travel from the injection site and cause adverse events, and that the spike protein, if biologically active, is very dangerous.”
That groundbreaking video was banned from YouTube.
In another bombshell discussion on Steve Bannon’s War Room podcast in July, Malone said reports showing that vaccinated people were carrying “higher levels of virus than previously understood” indicated that a worst-case scenario could be unfolding.
“This is precisely what one would see if antibody-dependent enhancement was happening,” Malone said. “What is antibody-dependent enhancement? Briefly, it’s that the vaccine causes the virus to become more infectious than would happen in the absence of vaccination, would cause the virus to replicate at higher levels than in the absence of infection.”
“This is the vaccinologist’s worst nightmare. It happened with the respiratory syncytial virus and in the ‘60s and caused more child deaths in vaccine recipients than unvaccinated. It happened with Dengvaxia, the dengue vaccine,” Malone continued.
“And it’s happened with virtually every other coronavirus vaccine development program, certainly in humans, known in history, and it’s what the vaccinologists like myself have been warning about since the outset, is the risk of antibody-dependent enhancement,” he said.
Malone told Bannon that ADE seemed most apparent in people injected with Pfizer’s vaccine. “So, we now know that the Pfizer protection is waning at six months,” he said. “And what the data seem to suggest is those who have received Pfizer, which is probably the least immunogenic of the three in terms of durability, length of protection, people that are now in the waning phase of the immune response to the Pfizer vaccine seem to be getting infected.”
“Notice they keep talking about Pfizer and not about the other two. So, this suggests this is exactly what you would anticipate, is the window of greatest susceptibility to antibody dependent enhancement is in this long tapering phase as the vaccine response declines,” he added.
“If the data are consistent with [antibody dependent enhancement], we have to stop the vaccine campaign,” Malone stressed. “We have to pivot to expediting as much as possible drug treatments, which have been largely blocked and suppressed at the FDA level, particularly for repurposed drugs.”
In an interview with the Epoch Times earlier this month, Malone questioned why Ivermectin, a drug that is used in other countries to combat the pandemic, and is available over-the-counter in countries like Mexico, has been declared a toxic horse dewormer in the United States.
“Why would the government be denigrating these agents that are known to be safe, been used for decades?” Malone asked.
In a recent tweet, Dr. Malone linked to a website that has been set up to report doctors who are spreading “disinformation” about COVID, in an attempt to have their physicians’ licenses suspended.
“This is what we’re up against,” he wrote.
During the Global COVID Summit in Rome, Italy, last month, Malone read a declaration—now signed by over 9,100 doctors and scientists from around the world—accusing COVID policy-makers of “crimes against humanity.”
You can follow Dr. Malone on Twitter @RWMaloneMD.
Dr. Peter McCullough
Dr. Peter McCullough, 58, is an internist, cardiologist, and epidemiologist who since the outset of the pandemic, has been a leader in the medical response to the COVID-19 disaster.
McCullough has been a vocal proponent of early intervention to treat COVID patients, publishing “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection” in August of 2020.
The doctor has 46 peer-reviewed publications on the infection and has commented extensively on the medical response to the COVID-19 crisis in media appearances. He is also a contributor to the conservative website, America Out Loud.
On November 19, 2020, McCullough testified before the U.S. Senate Committee on Homeland Security and Governmental Affairs on the pandemic. He also testified throughout 2021 before the Texas Senate Committee on Health and Human Services, the Colorado General Assembly, and the New Hampshire Senate concerning many aspects of the federal government’s response to the pandemic.
McCullough is an outspoken critic of that response.
“With this program, there is no critical event committee, there is no data-safety monitoring board, and there’s no human ethics committee,” he said during a webinar in June. “Those structures are mandatory for all large clinical investigations, and so the word that’s really used for what’s going on is malfeasance, that’s the wrongdoing of people in authority,” the doctor explained.
“Without any safety measures in place, you can see what’s going on. Basically it’s the largest application of a biological product with the greatest amount of morbidity and mortality in the history of our country.”
McCullough declared that the world has been subjected to a form of bioterrorism that has come in two stages—the first wave being the rollout of the coronavirus, and the second, the rollout of the dangerous vaccines, which he said may already be responsible for the deaths of up to 50,000 Americans.
The doctor gave a must-see overview of the pandemic in an amazing presentation last month in a church in Michigan.
In his talk, McCullough suggested that hospital policies are driven more by fear than by a commitment to helping people.
Based on conversations he heard between medical professionals early on in the pandemic, McCullough said it was clear that that “the biomedical complex” was more interested in protecting healthcare workers from getting infected, than in treating those sick with the disease.
“I was in on a lot of tactical calls for our center,” he explained. “And the calls went something like this: ‘Where do we get enough masks to protect ourselves, where do we get enough hazmat suits to protect ourselves, how do we get people on the ventilator early so we can cap off the air so the virus doesn’t spray all over the place. Let’s put the patients on the ventilators early.”
McCullough said that the discussions were “horrifying” to hear, and made it clear that medical institutions were not treating COVID patients adequately. By October of 2020, he said, the NIH set a “treatment standard” that discouraged any treatment for COVID patients until they were sick enough to go to the hospital. Then, when their condition was almost irreversible, they could be put on a ventilator, and given Remdesivir, he complained.
“I couldn’t stand it,” he said, adding that he began working “feverishly” with some colleagues in Italy to come up with an effective treatment for COVID patients. McCullough explained that in severe cases of the disease, there are three phases: viral replication, cytokine storm, and thrombosis.
“At first the virus is replicating like crazy, it trips off inflammation, and then that trips off blood clotting,” he said. In the end, according to the doctor, the patient gets micro blood clots in the lungs, and is unable to breathe. “The oxygen levels go down, the patient dies,” he explained.
Due to the complex nature of the virus, McCullough stressed that no single drug would be sufficient.
“We must use drugs in combination,” he explained. Last year, he noted that public health leaders insisted on having “large randomized trials” that take two to five years before any off-label COVID treatments could be used.
“That’s a long time, and it soon became obvious that the NIH was not interested in doing any randomized trials,” he said. The doctor pointed out that no other disease has been treated this way, where patients are sent home to fend for themselves.
McCullough developed an early treatment regimen for COVID patients to prevent them from having to go to the hospital, which he argues emphatically is the last place you want to go.
This video is almost 90 minutes long but is essential viewing for those interested in an intelligent and scientific counter-narrative to the conventional wisdom.
Dr. Michael Yeadon
No one has been more critical of the vaccines than Dr. Mike Yeadon, 60, a British physician who has a Ph.D. in respiratory pharmacology. Yeadon is a former vice president at Pfizer, where he also spent 16 years as an allergy and respiratory researcher. He later co-founded a biotech firm that a Swiss drugmaker purchased for around $325 million.
In a widely-viewed July interview with Del Bigtree, a filmmaker skeptical of the COVID vaccines, Yeadon stressed that he isn’t opposed to safe vaccines, only to vaccines he considers unsafe.
For the ensuing hour-and-a-half, Yeadon explained in great detail why he was so concerned about the COVID vaccines.
The doctor explained that he’s had a lifelong talent for spotting “patterns in sparse data,” which has served him well through life, especially when he was the CEO of his own biotech company. At the onset of the COVID pandemic, he said, this talent enabled him to realize “quite quickly” that what everyone was “being told about this virus and what we needed to do in order to stay safe was simply not true.”
For example, Yeadon said that there were immediately major changes in how the government attributed causes of death.
“We’ve never had anything so absurd as the rule that is now used that if you should die within 28 days of testing positive for COVID-19, then you would be declared as dying of COVID-19,” Yeadon said. “That’s just wrong. It’s not just a matter of disagreeing about something professionally, it is complete nonsense.”
The doctor said the lockdowns were also nonsensical because people who are contagious are sick, and stay home.
“So the idea that you cut normal contacts out at work, and civic society in a normal economy, that that would slow the epidemic spread I was fairly sure early on, that was bunk,” he said. “Basically, everything your government has told you about this virus, everything you need to do to stay safe, is a lie,” Yeadon said. The doctor also blasted the unreliability of the PCR testing, and the highly consequential claim that the virus could spread asymptomatically.
“Not one of those things is supported by the science,” he argued, adding that the lies have led us to “the very precipice of hell.”
Yeadon said that when he talks with fellow scientists, they privately agree with him that “PCR testing as it was being done was complete nonsense,” the lockdown was “clearly irrational and probably killed lots of people,” but unfortunately, “they were not willing to say anything about it in public” because the authorities at the universities did not want anyone questioning the government narrative.
“So that’s what happened,” he explained. “We ended up with people looking the other way.”
Yeadon said the reason he was speaking out was because “it’s not just my life, but more importantly that of my children and grandchildren that has been stolen from us by a systematic process of fear and control that’s going to culminate I think in some very horrible times, and I’m desperate to wake you up.”
“So when your government lies to you once or twice, we’re probably quite used to politicians on occasion telling white lies,” Yeadon continued. “But when they lie to you about something technical, something that you can check, and they do so repeatedly over months, and they do it over many, many elements of the same event—please, you’ve got to believe me—they’re not telling the truth, and if they’re not telling the truth, that means there’s something else afoot, and I’m here today to tell you that something very, very bad is happening, and if you don’t pay attention, you will soon lose the ability to do anything about it.”
In the July interview, Yeadon stated there was still a chance for people throughout the world to take their societies back from the clutches of the global medical establishment.
“You don’t need masks, they don’t work. Forget lockdowns—they never slowed transmission, which took place mostly in institutions like hospitals, and care homes. You don’t need to be vaccinated with inadequately tested and somewhat dangerous gene-based, spike protein-inducing proteins, and you don’t have to be told what to do by corrupt scientists who are apparently advising our government.” If you don’t do that for the next few weeks, he said, “it will be over.”
“I believe that if we get to the point of a so-called vaccine passport, I think you will have lost the chance to take it back, and you will regret it.”
Watch the entire video below to hear Yeadon expound on what he believes is afoot.
Dr. Ryan Cole
Dr. Ryan Cole, whose specialty is dermatopathology (the study of skin pathology), is also a board-certified pathologist and owner and operator of a diagnostics lab. He is known for calling the COVID vaccines “needle rape,” and for advocating alternative treatments for the virus.
Cole recently became a member of the Central District Board of Health (CDH), one of Idaho’s largest public health boards.
While speaking at a state of Utah-sponsored conference in May, Cole over-optimistically pronounced that the pandemic was over in the United States due to the low case numbers. Unfortunately, even as millions of Americans were vaccinated, cases skyrocketed throughout the summer, with no end in sight as new variants emerge.
During his talk, Cole championed the use of vitamin D to fight COVID-19, strongly recommending that people take the vitamin to boost their immune systems.
“There is no such thing as flu and cold season, only low vitamin D season,” Cole stated. He called Vitamin D “the master key to our immune health,” which can stop a cytokine storm. One reason obesity is a top comorbidity is that it “drastically reduces” the ability of vitamin D to get into one’s circulation. Cole called COVID-19, “a vitamin D deficiency pandemic,” and questioned why public health authorities, especially Dr. Anthony Fauci had not made a point of promoting the easily obtainable vitamin to help fight COVID.
Dr. Cole has also found an increase in cancers since the COVID-19 inoculation rollout.
On March 18, Cole reported to the public in a video produced by the Idaho state government’s “Capitol Clarity” project, that he is seeing a massive “uptick” in various autoimmune diseases and cancers in patients who have been vaccinated.
During an interview with Del Bigtree, he shared an anecdote from an Irish family doctor who has been in practice for 40 years.
“He knows his community, he knows his patients,” Cole noted, adding that the doctor told him that within a six-week period, he saw a vast number of vaccinated patients who have been presenting with cancers he’d never before seen in his long career.
The Idaho doctor also referenced a recent study conducted by researchers in the Netherlands and Germany that indicated the Pfizer-BioNTech vaccine “induces complex reprogramming of innate immune responses.” He said he discussed the uptick in cancer cases with renowned epidemiologist Harvey Risch, who told him that post-vaccine, “it’s usually five to 10 years before you see these signals.”
Cole said he argued that these vaccines are brand new and seem, according to the study, to be suppressing cancer-fighting receptors.
“All day long our cells are fighting off mutations in different cells. They see the mutation, they try to kill that cell,” he explained. “If this receptor is down-regulated, then all those downstream molecules inside that cell fighting there—it can’t fight because those signals are now turned off—the cytokines, the interferons, the things that will attack that atypical cell. So, we’re seeing the early signals of this.”
“Since January 1, in the laboratory, I’m seeing a 20 times increase of endometrial cancers over what I see on an annual basis,” reported Dr. Cole in the video clip shared on Twitter.
“I’m not exaggerating at all because I look at my numbers year over year, I’m like ‘Gosh, I’ve never seen this many endometrial cancers before,’” he continued.
Dr. Jessica Rose
Dr. Jessica Rose has been analyzing the data from VAERS (Vaccine Adverse Events Reporting System) and doesn’t like what she sees.
Rose has a bachelor of science degree in applied mathematics and a master’s degree in immunology. She completed her Ph.D. in computational biology at Bar Ilan University in Tel Aviv, Israel, a post-doctorate in molecular biology at the Hebrew University of Jerusalem, and is currently working on a post-doctorate in biochemistry at the Technion Institute of Technology in Haifa, Israel.
Rose spoke during the FDA’s open public hearing on September 17 to discuss whether or not to recommend booster shots.
“There’s an over 1,000 percent increase in the total number of adverse events just for 2021 and we are not done with 2021,” Rose said. “In my opinion [the risks] outweigh any potential benefits . . . with these products, especially in children.”
According to Rose’s analysis, a total of 551,836 adverse events stem from the Pfizer, Moderna, and Johnson & Johnson vaccines. The VAERS database as of September 25 showed a total of 97,149 severe adverse events, including 8,904 deaths, 33,172 hospital visits, 70,166 visits to the emergency room, 8,747 life-threatening reactions, 8,714 disabling events, and 323 birth defects.
“It’s alarming,” Rose said in a recent interview. “People need to stop denying that there’s something bad going on in terms of the adverse events associated with these products. There’s something bad going on.”
“These products are causing a large majority of these adverse effects,” Rose added. “You cannot deny that.”
Adam Gaertner
Adam Gaertner, an Arizona virologist, claims to be the first person in the country to discover the efficacy of Ivermectin for treating COVID.
He said in an interview on “Weaponized News” that in March 2020 he was researching how the virus works and discovered that similar viruses had been treated with a natural protein that could be produced with the help of interferons. Then he came upon an old paper that had mentioned ivermectin as a drug that could cause elevated levels of these interferons. Gaertner said he started networking with doctors on the use of the drug to treat COVID and found a physician in South America who had been treating COVID patients with ivermectin. He said the doctor had been using hydroxychloroquine on patients but the hospital had run out, so out of desperation they started offering other potential treatments to COVID patients.
“Ivermectin saved every single one of their patients,” Gaertner said.
He flatly stated that ivermectin prevents COVID if taken once a week, and is the cure for the disease.
Lately, Gaertner has been preoccupied with prion disease, a terrible neurological disorder that is 100 percent fatal.
He has been reporting his alarming findings on Twitter and on his blog Covid Candy.
According to Gaertner, the COVID spike proteins that are replicated by the vaccines in human cells are prions that can cause prion disease. Gaertner has been doing his own independent research on prion disease, compiling stories from people who have been diagnosed with the disease, or know someone who has it. The researcher says he’ll publish a report on his findings soon.
Dr. Lee Merritt
Dr. Lee Merritt, 67, completed an orthopedic surgery residency in the U.S. and served nine years as a Navy physician and surgeon before returning to Rochester, where she was the only woman to be appointed as the Louis A. Goldstein Fellow of Spinal Surgery.
Merritt has been involved in the private practice of Orthopedic and Spinal Surgery since 1995, has served on the Board of the Arizona Medical Association, and is past president of the Association of American Physicians and Surgeons (AAPS).
Merritt spoke at an America’s Frontline Doctors one-year anniversary event in July.
“There were only 20 deaths of all the active-duty military for all of 2020—in all the services put together,” she said, adding that the government is still pushing vaccinations on the troops.
“And we’ve already had tumors, and we’ve had 80 cases of myocarditis,” she continued. “The vaccine program has killed more of our young active-duty people than COVID.”
The doctor also noted that the VAERS database has shown a massive uptick in cancers.
“There’s 48 on average in VAERS, we’re now up to 229,” Merritt said. In 31 years, she added, there were 317 cases of myocarditis reported to VAERS. “Now, this year, there are 1,113,” she said on July 27. The doctor questioned why the government was continuing to push the experimental vaccines in the face of such dreadful data.
“In my opinion, I think you have to look at your worldview—if you think we’re fighting a virus, you’re going to act like a victim. If you think we’re fighting a war, you’re going to act like a warrior,” she said.
Dr. Merritt is convinced that the coronavirus was created in a lab, and the world is facing what appears to be biological warfare.
“It fails all of the cardinal signs of a natural disease,” she told Turning Point USA founder Charlie Kirk on September 7. “And the thing that worries me the most is we’re not treating it like we would any other pandemic.
When asked whether vaccine-hesitant people are right to be suspicious of the injections, Merritt was unequivocal.
“It’s striking to me that Americans would spend more time researching a new car before they bought one than taking a vaccine that’s made out of synthetic DNA, or synthetic RNA, and can change your genetic makeup forever. I mean, come on. This is serious stuff we’re dealing with here, and this isn’t a vaccine, it’s—we actually found a term for it—it’s a viral-based genetic therapy.”
Dr. Merritt told The New American‘s Alex Newman that it is impossible to know whether the Communist Chinese released the COVID-19 virus on purpose or by accident, but the implications are enormous. Merritt painted a dire picture for the United States if it doesn’t change course, and pointed out that there are ways to treat viral infections that are time-tested and effective.
Dr. Anne McCloskey
Dr. Anne McCloskey worked as a general practitioner in Derry, Ireland until she was suspended for speaking out against the vaccines.
Earlier this year, McCoskey posted a nine-minute video online in which she described treating the injuries of “damaged” people after they were given the COVID-19 injections, and advised people to not get vaccinated.
In her video, McCloskey said she witnessed numerous “sick, distressed, worried, traumatized” patients.
“Almost all of them, with the exception of small children, have been double jabbed,” said McCloskey, who referred to the COVID-19 injections as “an experimental genetic therapy.”
McCloskey added that some of the patients had been “coerced, bribed, or bullied” into getting the jab, and noted that in contrast to last year, hospitals and emergency departments this year have been “full,” despite many people having had “two doses of injections.”
“I’m seeing young people, healthy—previously fit young people—who are damaged, God forbid that it’s irreparably,” added McCloskey. One of her patients was a “young girl” with an upper arm blood clot, which McCloskey had “never seen” in a healthy young person in her “40 years of medicine.”
McCloskey said she also had as a patient a “young man” who had been “unable to get out of bed for two weeks” after getting his COVID injection.
“This whole hype has largely been a figment of the media, and the government and their lying scientific advisors and their deceptions,” stated McCloskey.
“Our NHS is being dismantled,” she declared, “it’s not overwhelmed, it’s being dismantled in front of our eyes.”
“I am not sleeping at night worried about what these injections are doing, because they’re certainly not improving the health and well-being of the community,” continued McCloskey.
McCloskey retired in 2019 after over 30 years of service, but returned to the forefront of the medical service last spring, when calls were made for increased numbers of health staff in light of the onset of COVID-19.
“We who look at real-world data, and have been studying this from the beginning, can see that this is not about health. These injections are doing real harm, they are certainly not providing any physical protection for people, and they are still in clinical trials for another two years,” McCloskey said.
She attacked the “false assumption” of there being no other treatments for COVID-19, which has allowed the experimental injections to be granted emergency use authorization, say it’s “chilling” to understand the “potential harms” the injections might have.
People around the world who have taken the injections “in good faith . . . have been lied to” stated McCloskey. “This must stop.”
“We need to stop this,” she added, referring to the vaccination drives. “We need to get the information out.”
“People are being harmed, and people are dying,” she warned.
Ireland’s Health and Social Care Board (HSCB) took a “very serious view” of her comments.
Northern Ireland’s Chief Medical Officer, Sir Michael McBride said he was “personally appalled” by her stance and that “the evidence on the effectiveness of the vaccines is irrefutable.”
Nearly 20,000 people have signed a petition demanding that the “well-known and popular GP” be reinstated.
Dr. Pierre Kory
Dr. Pierre Kory is an American critical care physician whose expertise is in critical care ultrasonography.
In 2015, Kory and his two co-editors won the British Medical Association’s 2015 President’s Choice award in medical textbooks for their work on Point of Care Ultrasound.
He was the critical care service chief at the University of Wisconsin Health University Hospital until May 2020, and later joined Aurora St. Luke’s Medical Center in Milwaukee, Wisconsin, before becoming a locum tenens physician. He is the president and co-founder of the Front Line COVID-19 Critical Care Alliance (FLCCC).
Kory gained notoriety in December of 2020 when he strongly advocated using off-label drugs like ivermectin for COVID-19 during a Senate hearing called by Senate Homeland Security Committee Chairman Ron Johnson (R-Wis.).
“In the last nine months in our review of all of the literature . . . we have done nothing but try to figure out how to identify a repurposed and available drug to treat this illness.”
Kory stated that he was “severely troubled” by the fact that the NIH, FDA, and the CDC have not assembled a task force to review repurposed drugs to treat COVID.
“Everything has been about novel and/or expensive pharmaceutically engineered drugs,” he complained. Kory testified that his organization, the FLCCC had found a solution to the crisis, namely the anti-parasite drug Ivermectin.
“There is a drug that is proving to be of miraculous impact. And when I say miracle, I do not use that term lightly.”
Kory stressed that he wasn’t being sensational. “That is a scientific recommendation based on mountains of data that has emerged in the past few months,” he said, adding that the NIH’s recommendation not to use Ivermectin outside of controlled trials was outdated.
“Mountains of data have emerged from many centers and countries around the world showing the miraculous effectiveness of Ivermectin. It basically obliterates transmission of this virus,” he testified.
Dr. Pierre Kory, MD testimony (con't)
Homeland Security Committee:
Focus on Early Treatment of COVID-19
Dec 8, 2020
More proof that the US government, in league with Big Pharma are trying to divert all money and attention to exotic unproven Pharma inventions and vaccines:
(2/4) pic.twitter.com/rFNhv8Oajq
— Patrick Henningsen (@21WIRE) December 11, 2020
Testimony of Dr. Pierre Kory, MD
Dec 8, 2020
Real proven therapeutics for #COVID, rather than 'new' experimental vaccines and drugs…
(4/4) pic.twitter.com/crQRG52meb
— Patrick Henningsen (@21WIRE) December 11, 2020
Dr. Vladimir Zelenko
Dr. Vladimir Zelenko is a board-certified family physician who provided counsel to Trump White House personnel in 2020, as well as multiple governments, hospitals, and physicians.
Dr. Zelenko was born in Kiev, Ukraine, and grew up in New York City. He earned his M.D. from the State University of New York at Buffalo.
Fairly early on in the pandemic, the doctor developed protocols for low, moderate, and high-risk patients to treat COVID-19, and their use as prophylaxis against the virus.
Zelenko spoke with author John Leake about how he successfully used hydroxychloroquine to treat patients with COVID-19 and then later shared his insights with the Trump White House.
After President Trump embraced Zelenko’s treatment protocol, government agencies such as the NIH and FDA dismissed it, and prevented public access to its key ingredient, hydroxychloroquine. Zelenko argues that this deliberate suppression of a life-saving medication led to the preventable deaths of hundreds of thousands of Americans.
Dr. Joseph Ladapo
Dr. Joseph Ladapo became Florida’s new surgeon general on September 21.
Ladapo graduated from Harvard Medical School in 2008 and received a separate doctorate that year in health policy from the university’s Graduate School of Arts and Sciences, according to a statement from Florida Governor Ron DeSantis’s office.
“His national honors include the Daniel Ford Award for health services and outcomes research, and he was also a regular columnist for the Harvard Focus during medical school and residency, where he discussed his experiences on the medical wards and perspectives on health policy issues,” DeSantis’s office said.
Ladapo says the state should not be making public health decisions out of fear, and that vaccination mandates are not the answer to the coronavirus pandemic. Vaccination should be a choice, he told reporters during a press conference last month.
“The state should be promoting good health,” he said. “Vaccination is not the only path to that. It has been treated almost as a religion. That is just senseless. There are lots of good pathways to health, and vaccination is not the only one.”
Gov. Ron DeSantis announced Ladapo appointment following a meeting of the Florida cabinet. Ladapo is replacing Dr. Scott Rivkees, whose last day was Monday. Rivkees has not been seen or heard from publicly since the early days of the pandemic.
Ladapo was also critical of school closures and quarantines, saying ‘we’ve just brazenly pulled children who need the structure of school and routine in their lives, out of school. And we’ve done that . . . it’s terrible to do it for all kids, but we’ve also done it for kids with disabilities, and people have hardly batted an eye.’
Ladapo’s publicly stated positions are similar to those of DeSantis and his informal advisor, Dr. Jay Bhattacharya. Both Ladapo and Bhattacharya are signatories to a document called the Great Barrington Declaration which rejects most of the current COVID-19 mitigation policies and calls for a more focused approach.
“He has had both a remarkable academic and medical career with a strong emphasis in health policy research,” said DeSantis in a statement. “Dr. Ladapo will bring great leadership to the Department of Health.”
Dr. Dan Stock
Dr. Dan Stock is a licensed primary care physician who irked medical elites when his address to the Mt. Vernon School Board in Indiana panning mask mandates and COVID-19 protocols became a viral video.
According to his LinkedIn bio, Stock is a physician at PureHealth Functional Family Medicine in Noblesville and is also the center medical director for Grifols Plasma, a global healthcare company with 24,000 employees in more than 30 countries and regions. Prior to this, he was a physician at Activate Healthcare in Anderson and a lecture bureau speaker for 24 years at Liposcience.
During his remarks in front of the school board on August 6, 2021, Stock said that the reason the country was still in a pandemic was that “we are doing things that are not useful, and we’re getting our sources of information from the Indiana Board of Health and the CDC who actually don’t bother to read science before they do this.”
Stock continued: “I am especially trained in immunology and inflammation regulation, and everything being recommended by the CDC and the State Board of Health is actually contrary to all the rules of science.”
Coronavirus and other respiratory virus particles are small enough to go through masks, Stock argued. He also cast doubt on the efficacy of the vaccines, pointing out that the virus was on the rise in the middle of summer, a time when respiratory viral syndromes are typically at their lowest.
The doctor made note of the COVID-19 outbreak in Provincetown, Massachusetts, which struck almost entirely vaccinated individuals.
“Vaccines don’t prevent infection, just symptoms,” Stock said. “So you cannot stop the spread, you cannot make these numbers that you’ve planned on get better by doing any of the things that you’re doing,” he said. “Because that is the nature of viral respiratory pathogens. And you can’t prevent it with a vaccine because they don’t do the very thing you’re wanting them to do. And you will be chasing this through the remainder of your life until you recognize the Centers for Disease Control and the Indiana State Board of Health are giving you very bad scientific guidance.”
Dr. Harvey Risch
Dr. Harvey Risch is a professor of epidemiology in the Department of Epidemiology and Public Health at the Yale School of Public Health and Yale School of Medicine. Risch testified at a November 19 Senate hearing on the use of hydroxychloroquine as an early treatment for COVID-19 patients.
About studies of hydroxychloroquine early use in high-risk outpatients, every one of them, and there are now seven studies, has shown significant benefit: 636 outpatients in São Paulo, Brazil; 199 clinic patients in Marseille, France; 717 patients across a large HMO network in Brazil; 226 nursing-home patients in Marseille; 1,247 outpatients in New Jersey; 100 long-term care institution patients in Andorra (between France and Spain); and 7,892 patients across Saudi Arabia. All these studies pertain to the early treatment of high-risk outpatients—and all showed about 50 percent or greater reductions in hospitalization or death. The Saudi study was a national study and showed 5-fold reduction in mortality for hydroxychloroquine plus zinc vs zinc alone. Not a single fatal cardiac arrhythmia was reported among these thousands of patients attributable to the hydroxychloroquine. These are the non-randomized but controlled trials that have been published.
Dr. Craig M. Wax
Dr. Craig M. Wax is a family physician from Mullica Hill, New Jersey who advocated an early treatment regimen to treat COVID-19 in the spring issue of the Journal of American Physicians and Surgeons.
Wax described in the article how he had become very ill with COVID-19 despite following stringent mask-wearing and social distancing recommendations. He described his experience and his early home treatment regimen, in the spring issue of the Journal of American Physicians and Surgeons.
The Associated Press covered his story in an article in March.
When he first suspected the diagnosis, he continued his daily regimen of multivitamins/multi-mineral supplements, vitamin D3 5,000 IU, and vitamin K-2 180 mcg; added N-acetylcysteine (NAC) 600 mg daily; increased his hydroxychloroquine from 200 mg weekly as prophylaxis to 200 mg twice daily and zinc to 220 mg (50 mg elemental) per day; added azithromycin 250 mg twice daily; and then added ivermectin 15 mg daily in sequenced multi-drug early home therapy.
When symptoms continued to worsen, he consulted colleagues who recommended adding a tapering dose of prednisone starting with 30 mg a day and aspirin 325 mg daily. ‘Over two exceedingly difficult nights, the tide turned,’ he writes. By day 12, he could resume his daily strenuous outdoor bicycling.
In contrast, the physician from whom he probably acquired the infection received little pre-hospital treatment and had an extremely severe course, including six weeks on a ventilator, Dr. Wax reports.
“This is just one example of the superior outcome with early home treatment versus therapeutic nihilism (‘stay home and come to the hospital if you worsen’),” he wrote. “Therefore, it is critical that physicians and patients are not only free to use new medications, but free to use any and all repurposed old medications, vitamins, minerals, exercise, and nutritional strategies.”
Wax emphasizes the importance of a healthy lifestyle, but warns that even low-risk persons may be severely affected by this disease. This is likely due to yet unconfirmed risk factors like blood type, A, B, or AB versus O.
“We have more than 12 months of experience with this disease, and why haven’t we spent more time on risk factor stratification, especially for isolation and other preventative strategies?” Wax asked. “Why did federal and state governments mandate methods of isolation for all, at risk of compounding commonplace morbidity and mortality for the population at large?”
“Unfortunately, governments, politicians, media, medical organizations, hospital health systems, pharmaceutical, and other industry interests have worked to hamper early treatment and block access to repurposed generic medications like hydroxychloroquine and ivermectin,” he concluded.
In an “open letter” to the White House, CSC, FDA, HHS colleges and universities and all others mandating the experimental vaccines, demanded answers to a series of questions regarding their handling of the pandemic.
Dr. Geert Vanden Bossche
Geert Vanden Bossche has a Ph.D. in virology at the University of Hohenheim, Germany, and has held adjunct faculty appointments at universities in Germany and Belgium. He has also worked in R&D and vaccine development for GSK, Novartis, and Solvay Biologicals. Bossche also served as a Senior Program Officer for the Gates Foundation’s Global Health Discovery team, and from there went to the Global Alliance for Vaccines and Immunizations (GAVI) and was the Senior Ebola Program Manager.
After that, he joined the German Center for Infection Research as head of the Vaccine Development Office, and currently works as a consultant on biotech/vaccine issues.
In March, Bossche put out an “urgent call” to the WHO on behalf of humanity to reconsider its push to impose mass vaccinations throughout the world because the vaccines, he said, were driving “viral immune escape.”
He said the policy of “ignoring or denying the [negative] impact of stringent infection prevention measures combined with mass vaccinations using prophylactic vaccines is a colossal blunder.”
“Please, do listen to my cry of distress,” he pleaded. “Let’s meanwhile devise a strategy to eradicate emerging, highly infectious variants.”
In June, a frustrated Bossche returned to YouTube for one last cri de coeur, after vowing to sit back and watch the disaster unfold since no one listened to his warnings. But when the global medical establishment voiced its intention of vaccinating children, he was spurred to speak out one more time in protest.
In a long post on his website last month, Bossche explained in detail how he believes the vaccines are generating the variants to disastrous effect:
Initially, people were told that ‘the more you vaccinate, the more you will prevent mutants from being generated and the less more infectious variants will spread’. This mantra proved miserably wrong as not only viral spread has increased in a number of countries despite very high vaccine coverage rates but it has now also become clear that the vaccinated spread the virus as much as the unvaccinated do (whereas it is even highly likely that vaccines are a more important source of transmission of naturally selected, highly infectious variants). Sadly enough, even a number of MDs have joined the club of fact checkers and have been taking advantage of their titles and reputation to divulgate simplistic and erroneous interpretations of the effect of mass vaccination campaigns. I cannot emphasize enough that, although none of them combine sufficient knowledge of virology, immunology, vaccinology and evolutionary biology to be able to understand what is driving the evolution of these pandemics towards a disastrous outcome, they have engaged in vilifying attacks that excelled in arrogance but were never built on solid scientific grounds.
He argued that the only way to undo the damage of the mass vaccination campaigns is to reach herd immunity, and explained in detail on his website how to go about doing that.
The Vaccine Superspead Hypothesis
the vaccinated superspread hypothesis
assessing the riddle of more recovered, more vaccinated, and more dying despite a lower CFR variant
 |
there has been a strange riddle in the covid data of late.
we have a lower CFR variant of the disease that has become predominant. delta has roughly 1/3 the case fatality rate of prior variants (like alpha)
far more people have acquired immunity from having had and recovered from covid. this immunity is long lasting and extremely effective. (much more so than vaccines)
high risk cohorts were significantly reduced last year. there is less “dry tinder” now.
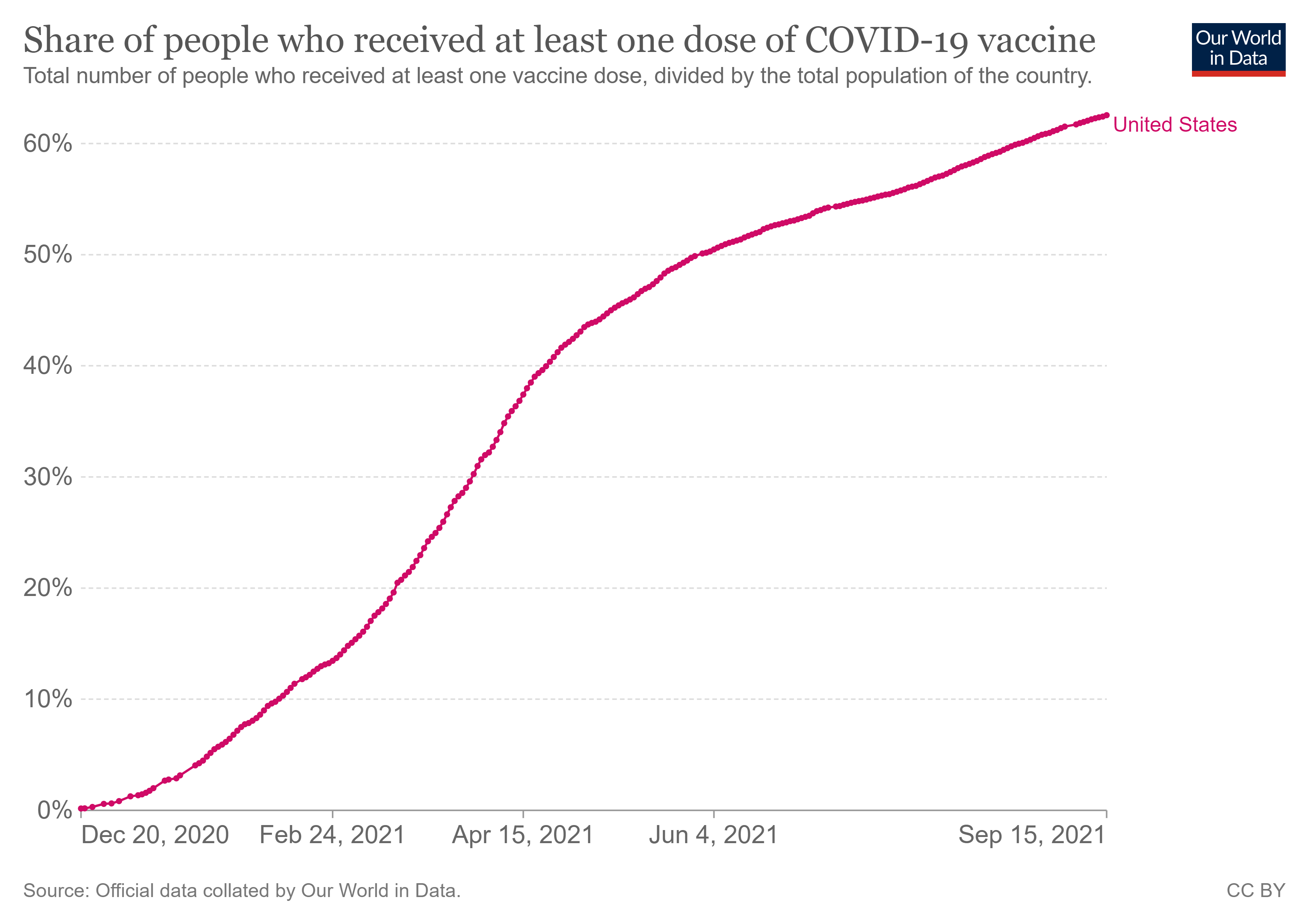
we have FAR more people vaccinated now. it’s 50-90% in many places and in many high risk groups. last year it was zero.
and yet in many of the high vaccine uptake places, we’re seeing deaths from covid (and excess mortality) rise to levels ABOVE last year.
this has led many to posit that vaccines not only don’t work, but that they make you worse.
but on an individual level, this does not appear to be true. (though there is quite a lot of evidence that vaccines induce higher risk in the two weeks post administration and that this is being accounted for dishonestly, added to the “unvaccinated” butcher’s bill, and artificially enhancing reported VE.
BUT, even if we control for this, vaccines are showing efficacy in preventing deaths among the vaccinated. it’s more like 50% than the 90%+ being claimed, but VE against death in the 50%’s should still be showing BIG community effects with so many people in the high risk groups vaccinated.
but, on a societal level, it’s not. we’re seeing breakouts to new seasonal highs vs last year and epidemics in covid death rapidly following vaccination campaigns. (MORE)
all else equal even without vaccines, we’d expect to see attenuation in covid deaths for the reasons laid out above. instead we see acceleration.
the case rate in covid would need to be 3X last year to drive equivalent deaths and higher than that to show excess. but, it’s nothing like that, especially once you control for testing levels.
this is showing up in excess deaths as well as covid deaths, so the signal looks real.
the data has caused a lot of hand wringing and confusion.
grab a seat, because i have an idea to inject into the debate, i sincerely hope that i am wrong, and i suspect a fair few folks are not going to like hearing it, but it’s the best fit i can find for the data.
so here we go:

the current surge in covid deaths is caused by the vaccinated.
the covid vaccines are extremely leaky and may well accelerate contracting and carrying covid.
they allow for very high viral loads to go unnoticed and generate a new and severe asymptomatic spread vector to where none existed before.
the high viral loads lead to greater contagion. they may lead to greater severity (but this data is iffy and contested)
vaccine campaigns cause superspread events because vaccination leads to a 2 week window of 40-100% more covid risk that then gets counted as “unvaccinated” because the definitions are bad.
this combination makes those vaccinated with one dose or more into superspread bombs.
you get a surge of spread that gets misallocated (and used to inflate VE) and then you get the later breakthrough cases (because the vaccines do not stop infection and just mitigate severity)
these BT cases have massively high VL in often asymptomatic superspreaders that pass on high loading doses to the unvaccinated and greatly worsen the overall pandemic.
this further inflates apparent VE by subjecting the unvaccinated to a more profligate and severe disease vector than they would have been had no vaccination campaign ever been undertaken.
it moves the whole system to a a different valence.
perversely, if the vaccinated comprise a spread vector that accelerates deaths in the unvaccinated, that would make it look like vaccines work.
ouch. (told you you weren’t going to like it)
in the longer run, this would also select for hotter, deadlier strains because that’s what leaky vaccines do. (more HERE) this would really make life worse for everyone.
i want to stress, this is a hypothesis and a work in progress. it’s just the best fit to the facts i can find right now and i REALLY hope it’s wrong because if it’s right, this vaccination campaign is probably the worst health blunder in human history and the epidemiology and politics of that will get stunningly, surreally bad.
but if this hypothesis proves out, then calling this an “epidemic of the unvaccinated” is 180 degrees wrong.
it would mean that the unvaxxed are being assaulted by the vaccinated because this vaccine program was incredibly ill conceived and the vaccines are not suited to task and that it, quite literally, was the vaccination programs themselves that have re-intensified what should have been a waning pandemic.
if this validates, it’s not the unvaxxed threatening the vaxxed, it’s the vaccinated threatening everyone.
OK. that’s a lot to claim and there are a lot of hotlinks and cites above, but let’s add some more data to flesh this out.
we’ve seen the spikes in a great many places. they tend to follow vaccination pushes.
we know that vaccines are non-sterilizing and do not stop infection.
we also know that fully vaccinated doctors were carrying VL’s 251X those of prior variants.
and many of them were asymptomatic. what this study did not assess was “did this vary between the vaccinated and the unvaccinated?” we could not tell if it was a property of delta or of inoculation status.
but this study sheds some light and that light looks to support the idea of this new and potent asymptomatic spread vector where none existed before.
here is the key finding: look at asymptomatic. i’m eyeballing, but did use a tool to do it, so it looks like a 3-4 Ct variance for vaxxed vs unvaxxed. each cycle is a doubling. so that’s a 8-16X variance in viral load. that’s the evidence we’ve been looking for and we ought to be doing A LOT more studies like this one to see if this proves out.

some have criticized this study for not expressing overall prevalence of cases in vaxxed vs unvaxxd, but the UK variants of concern data does this for us and show the vaxxed actually running at higher infection rates when we adjust for cohort size.
so i find the “well, the vaccines would be prophylactic on spread” argument fraught. the data does not support it.
others have countered with data like this from the FT (who have been frankly terrible on data all covid and seem to make up half of what they publish) but let’s take it at face value.
first off, it’s easy to see the rigging of the reporting. you can see the lag while they wait for the enhanced vulnerability right after dosing to clear. this is more bunker reporting.

meanwhile, societally, we see this.

and we see this below despite a 2/3 lower CFR variant, more natural immunity accumulation, depleted high risk cohorts, and a high vaccination rate. (data will be messy this week for yom kippur but next week should be useful)

the idea that this data is evidence that “vaccines are working at a societal level” seems increasingly iffy. but the fact that they do seem to show some efficacy (even fully loaded with the high risk period) on the individual level yet seemingly accomplish the opposite societal scale needs to be explained.
it looks to me like “the vaccinated become a superspread vector and re-kindle and re-intensify the pandemic” fits all this data and it’s very possible that "your vaccine does not only not protect me, it may put me at greater risk.”
and you can see spreads like this all over.
look at the US aggregate data. see the weird shelves that break the gompertz pattern starting in mid feb?
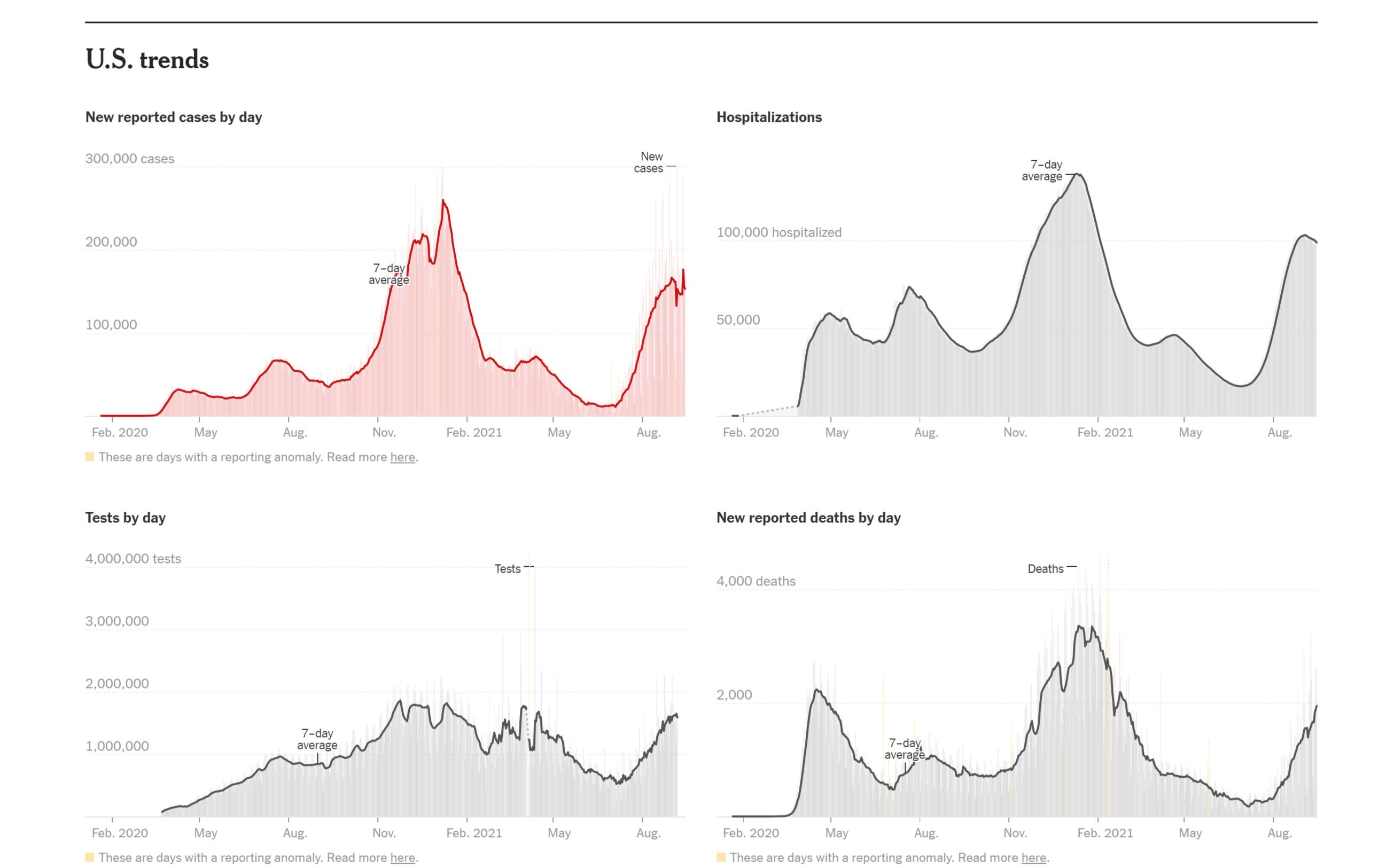
because that break in pattern lines up with this with just the sort of small lag you’d expect.
and now we’re seeing this as we look to be accelerating on all cause deaths despite all the vaccination and all the prior immunity, risk culling, and improvement in treatment and despite a far less deadly variant.
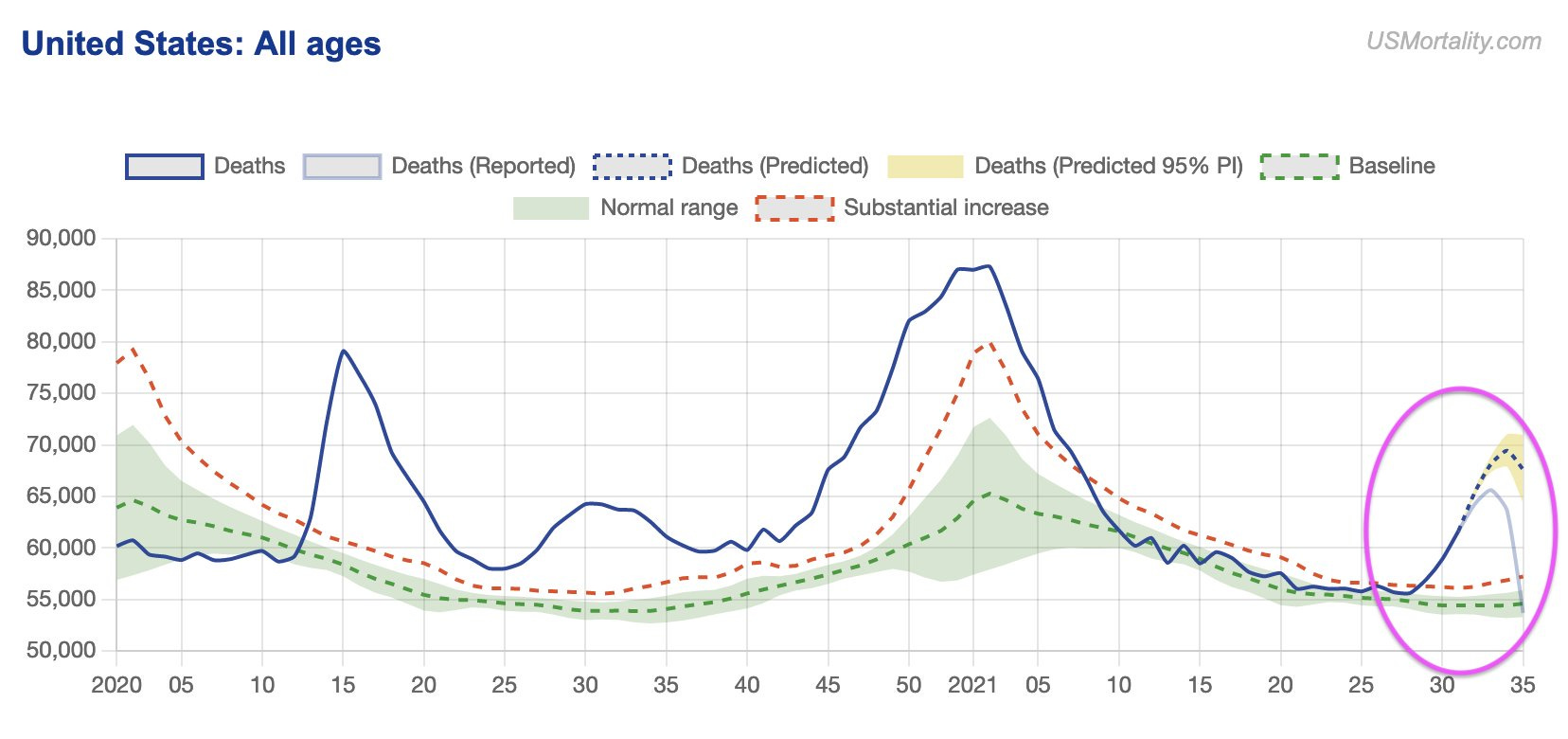
it’s even clearer in places that are already on the downside of seasonal surge and in vulnerable age groups (interestingly enough, with 85%+ vaccination rates).
this is DEEPLY counter to expectation if vaccines are working on a societal level or even from a world with no vaccines at all.

so, that’s the hypothesis.
i realize it’s provocative and not what people want to hear.
but i can find no better theory that fits all the facts. so, i send it forth into the world because maybe one of you can (and i really would like to be wrong here).
have at it. tear into it. find some contradictory data or a better explanation.
let’s do some science.
but your science must account for higher deaths despite more immunity and more vaccination from a variant with 1/3 the CFR that is nothing like 3X as prevalent.
it must explain surges in deaths following surges in vaccination.
it must explain apparent ~50% VE to the individual on deaths, but negative VE to the society as a whole around mass vaccination.
and for the love of francis bacon, please no appeals to authority. that’s laughably absent here.
the fact that we can even be seriously entertaining this issue underlines the reasons that vaccines, especially totally new modalities never before used in humans and with a laundry list of past safety and efficacy issues, undergo 6-10 years of study not 3-6 months of truncated and slanted review before being rolled out.
this has been a wild aberration in terms of practice and abrogation in terms of safeguards.
and they clearly got A LOT of this wrong.
remember the claims that the vaccine WOULD be sterilizing and stop infection and thus provide the backbone of herd immunity? they sure missed on that one.

it’s remarkable that having literally predicted 95%-100% mitigation in cases and gotten “cannot distinguish from 0%” that none of these “experts” or “authorities” have changed their policies or prescriptions.
hard to see that as “playing on the level” or “changing you mind as new evidence emerged.”
but that’s where we need to play if we want to get at the truth, even if it’s not a truth we want to hear.
vamanos.
(and
Subscribe to:
Posts (Atom)
Popular Posts
-
Dr. Vladimir “Zev” Zelenko is the Doctor who recommended that President Trump take hydroxychloroquine -Zelenko Protocol innovator: 99%...
-
Source by Fauna on Tuesday, May 24, 2011 From NetEase : Infant’s body atrophies after getting BCG vaccine [against tuberculosis], CDC says ...
-
Source (NaturalNews) The establishment mainstream media continue to parrot the same hysteria regarding the Zika virus – that it's caus...
-
Source There have long been suspicions over the levels of toxins in make-up, with numerous reports paying close attention, in particular...
-
Neurocysticercosis, infection with pork tapeworm larvae brain parasites, is an increasingly serious public health problem in the United Stat...


